
A few weeks ago I was chatting to a friend of mine on skype when, out of the blue, I was asked to give my opinion of the Coalition’s NHS reforms. For whatever reason, be it the fact that the NHS has been off the front pages for a while, cosmic rays interfering with my brain, the complexity of the issue at hand or simply me having a bad day, something odd happened. I found myself in a panic with once fresh and well-resourced arguments fading before me as I reached out for them, leaving, I’m quite sure, an incoherent and blustering crapsicle of an explanation for my poor comrade to attempt to absorb (that’s assuming she even bothered given the air of incompetence I’m sure it aroused).
This perturbed me a not inconsiderable amount. Like Napoleon, I rely all too heavily on the Vielle Garde of my memory sometimes, and I resolved to rally the fleeing squadrons and re-join the battle in blog form after gathering the necessary stratagems. OK? For simplicity and clarity’s sake, I’m not going to talk about the impact of the £20bn ‘efficiency savings’ (that is, cuts) to the NHS which are already wreaking havoc and instead focus entirely on the structural reforms. OK. Here we go.
An intro by a man with a stunning ‘tash (I think Biology students from my year will recall an all too personal video starring Prof Bob)
Flawed pretext for reform
Keeping things very clear, there are two ways to evaluate the performance of the healthcare system: cost and quality. Muddying the waters slightly, one could combine these factors and come up with the notion of cost-efficiency, or units of comparable-quality healthcare provided per £ spent. Maths students may prefer to think of it as a function of volume of care multiplied by a function of quality of care all divided by £.
The supporters of private commissioning (henceforth called privatisation) argued that the NHS performs poorly in terms of both cost and quality. In an age of austerity and an ageing population, so the argument goes, the NHS must change with the times in order to deliver the service we demand on a tighter budget.1,2,3
But as a study in the Journal of The Royal Society of Medicine concluded, the argument that pro-market reforms will enhance cost-effectiveness does not stack up.4 ‘The government proposals to change the NHS are largely based on the idea that the NHS is less efficient and effective than other countries, especially the US. The results question why we need a big set of health reform proposals … The system works well. Look at the US and you can see where choice and competition gets you. Pretty dismal results.’
But of course, one study proves nothing. In addition The King’s Fund’s analysis5 of NHS performance 1997-2010 found that:
- Hospital waiting times reduced dramatically from 1997-2010, with more than 90 per cent of patients waiting less than 18 weeks for treatment last year.
- Infant mortality has fallen and life expectancy is increasing for all social groups.
- Smoking rates have fallen, and deaths from cancer and cardiovascular diseases have been steadily declining.
- Infection rates for MRSA and C. difficile have been significantly reduced, and there are now robust systems for collecting and analysing information on adverse events.
- In mental health services, access to specialist early intervention and crisis resolution teams is considered among the best in Europe.
Still not convinced? How about this chart from The Commonwealth Fund6
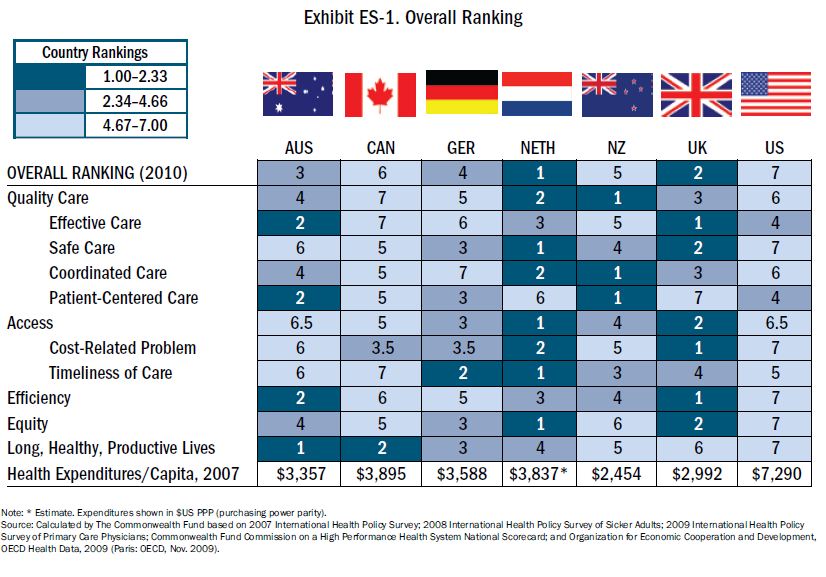
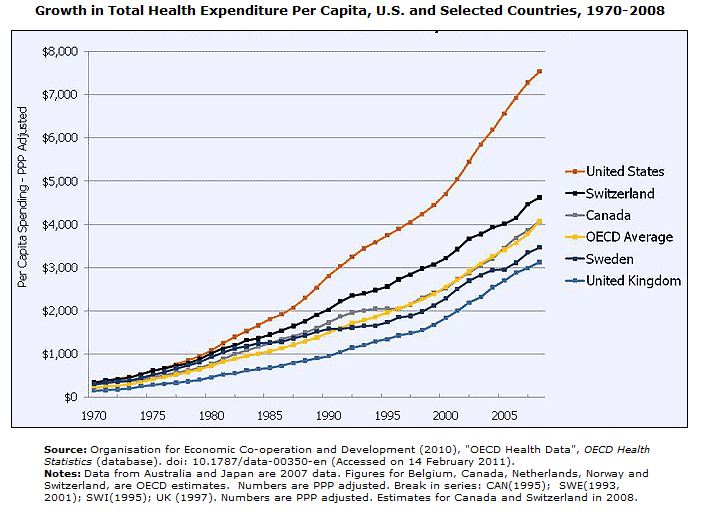
Or this from Kaiser Permanente7?
What about the cancer survival rates the Tories were so fond of referencing?
David Cameron and Andrew Lansley’s repeated criticisms of the NHS’s record on cancer have been contradicted by new research that shows the health service to be an international leader in tackling the disease.
The findings challenge the government’s claims that NHS failings on cancer contribute to 5,000-10,000 unnecessary cancer deaths a year, which ministers have used as a key reason for pushing through their radical shakeup of the service.
In fact, the NHS in England and Wales has helped achieve the biggest drop in cancer deaths and displayed the most efficient use of resources among 10 leading countries worldwide, according to the study published in the British Journal of Cancer.
“These results challenge the feeble justification of the government’s changes, which appear to be based upon overhyped media representation, rather than hard comparable evidence. This paper should be a real boost to cancer patients and their families because the NHS’s performance on cancer is much better than the media presents. It challenges the government’s assertion that the NHS is inefficient and ineffective at treating cancer – an argument for reforming the NHS,” said Prof Colin Pritchard, a health academic at Bournemouth University.8
So, putting it bluntly, there’s a bloody good reason why at the end of Labour’s term public satisfaction with the NHS was at a record high. Whilst there are obviously legitimate criticisms to be made and room for improvement, investment in health paid off in a swathe of across the board achievements9.
Ulterior motives
It might be worth noting that the biggest cheerleaders of reform were almost all either personally to gain through work for private health companies, or ultra-conservative extremists. These were the sort of ideological zealots who casually referred to the NHS as ‘a 60-year mistake’, and called for the ‘de-nationalisation’ of a ‘fundamentally broken machine’10,11,12,13,14.
As one eloquent crypto-fascist said ‘NFR has long argued that the NHS is an essentially Stalinist, nationalised abhorrence and that Britain can do musch [sic] better without its so called ‘principals’ [sic].’
Somebody needs spelling lessons!
Behind the scenes of course the CEOs of the circling private vultures were barely holding back their drool. Loosely worded press-releases like ‘we are entering a new, exciting era, driven by the forthcoming healthcare reform that will ultimately change, to our benefit, the landscape in which we operate’ or Tory advisors telling a room full of healthcare executives that ‘The NHS will be shown no mercy and the best time to take advantage of this will be in the next couple of years’ belied a key motive for the reforms. Bupa would like their shareholders to know all about ‘Medical insurers overview on the emerging NHS private sector’. The ‘NHS private sector’. Says it all really! 15,16,17
All this in addition to the 200 or so (mostly Coalition, but some New Labour) MPs and Lords with personal financial interests in private healthcare18.
Understanding the reforms
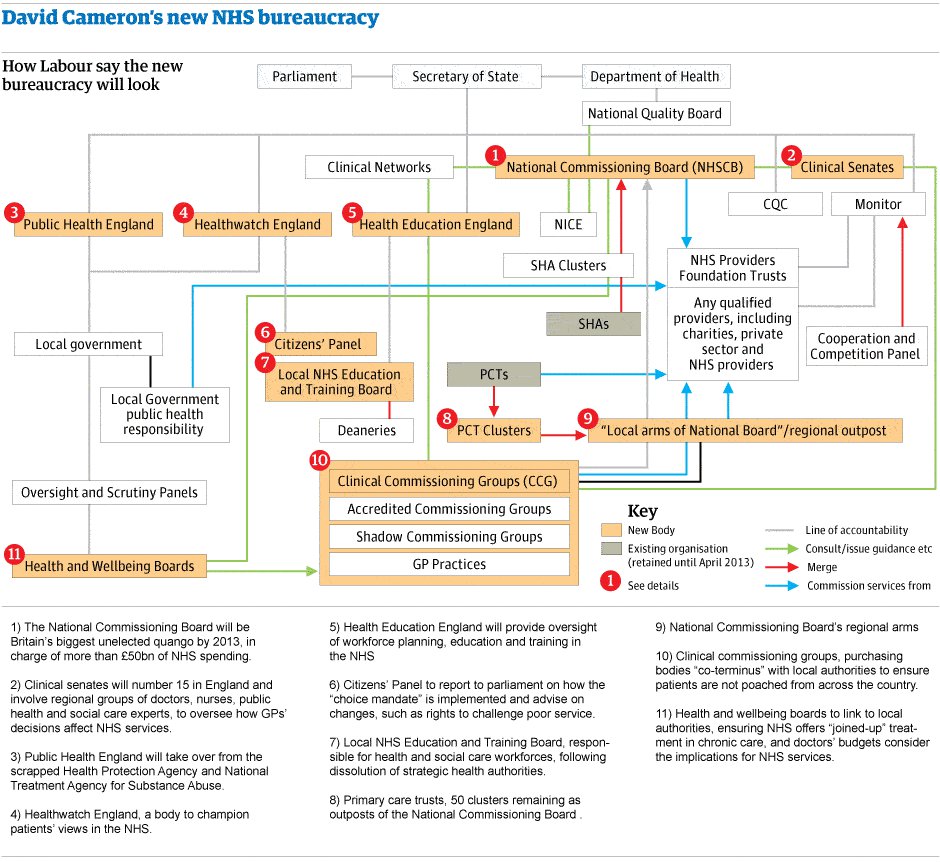
click to enlarge… if you dare
In other words, it’s a bit of mess. In fact, it’s harder to understand than a poorly translated Japanese instruction manual. Luckily for you, I have spent a good few hours researching the ins and outs of the changes and will now serve it up to you, semi-pre-digested-baby-food-style, in easily comprehended chunklets, accurate to the best of my time, knowledge and ability. Having said that I’m only human and there will probably be the odd mistake. Anyway, here goes.
The current system is (relatively) simple. The overall strategy of the NHS is derived by the Department of Health (DH). At a regional level, Strategic Health Authorities (SHAs) implement that strategy as well as ensuring the coherent adoption of regional directives. The SHAs do this in partnership with Primary Care Trusts (PCTs) at the local (e.g. county) level. Care is commissioned (aka purchased (aka NHS money spent on patients)) almost entirely by PCTs from NHS hospitals and GPs. NHS hospitals come into 2 categories, Hospital Trusts (HTs) and Foundation Trusts (FTs). HTs are the more ‘traditional’ model of NHS hospital and are run according to the wishes of the SHA. FT status is granted upon request to the most successful HTs and allows them greater independence from the SHA. FTs, by the way, do not exist in Scotland and Wales, and outside of England the system as a whole is independent of Westminster (lucky them!). You may want to read this paragraph again or refer back to it if all the acronyms get too much for you later on!
So little Johnny feels ill. His mum thinks it’s the flu, but takes him to the GP to get him seen to just in case. The GP is paid by the PCT to say hello to little Johnny and, woe is us, Johnny turns out to have Meningitis and is rushed to the local hospital and is treated within the overall acute care budget that the hospital has been given by the PCT. The way he is treated is influenced by DH/SHA policy to a greater or lesser extent depending on if it is an HT or FT. Thankfully, his life is saved but he appears to be paralysed by the Meningitis. He goes through physical therapy at the outpatient clinic of the hospital. He regains some motor function but still needs help with his day to day life. The PCT and SHA co-ordinate with the Local Council to transfer Johnny out of the NHS system to the social care system (currently run by Local Councils/Authorities (LAs) and having its budget hacked away at too). OK? That’s the chain of money and authority.
Starting in April 2013, PCTs and SHAs will be done away with altogether. I’m going to try to explain what replaces them, but bear in mind that I’ve had to simplify this a tad, because alongside the big organisations I’m going to mention, there are a crap load of smaller bureaucratic entities which absorb one role or another and support/advice/consult.
The SHAs’ role will be passed over to smaller sub-national and area offices, 54 of them in total (!), of the new National Commissioning Board (NHSCB). These offices will probably end up employing fewer people overall in strategic health than the 10 SHAs they replace. It’s likely that they will be largely ineffective in maintaining some sort of health strategy in the increasingly fragmented NHS they’re meant to guide since their role, according to the DH, is mainly to provide ‘leadership’ to local Clinical Commissioning Groups (CCGs, more on them in a bit), whatever that means. Presumably asking them very nicely not to take our lunch money.
But the mess in removing SHAs pales into insignificance when compared to the havoc that will be caused by the big change of the reforms: the abolition of PCTs. The PCTs are responsible for portioning out the lion’s share of the NHS to budget between hospitals, GPs and specialist care, as well as public health (ie community health, environmental health, epidemic control, safe sex, wash yer hands you dirty so and so, quit smoking campaigns and the like, that sort of jazz). So, where’s all this money going to be spent in the new system?
Well, starting in reverse order, public health budgets with go to local councils. I don’t really have much of an issue with this, providing the knowledge and experience is there in the councils, and the money remains ring-fenced as the Coalition claim it will be. Now I personally think public health is extremely important in the long term and I fear that if the money ever becomes available for cash raids then councils, Labour and Tory, will be falling over themselves to cut public health budgets as a politically easy cut to make. But basically, no complaints here. Moving on…
The commissioning (remember, this means buying or paying for) previously done by PCTs will now be done mostly by ‘consortiums’ of local GPs offices called Clinical Commissioning Groups (CCGs) and to a lesser extent by the NHSCB (that’s the SHA replacement). The NHSCB will be in charge of specialist budgets like dentistry and pharmacy and little will change except that certain things are being decommissioned entirely (such as primary care services for the homeless and other people not registered with a CCG), and that I would guess a local body like a PCT would better understand how dentistry works in their area than an office of 4500 people in Leeds.
Instead, the major problems of the changes are to be found in the CCGs and hospitals. The GPs practices which will make up the new CCGs have absolutely no existing infrastructure for doing commissioning. They don’t have the time, the staff, the facilities, the experience or the money. But the DH is, in April 2013, going to hand them the money. Loads of money. The GPs, who are not managers but clinicians, are expected to become accountants as well as doctors. So, as the DH has reluctantly accepted, they will simply outsource their commissioning. This will mean a swathe of new private sector commissioning companies, many of which will be staffed by old PCT and SHA staff (makes sense, given they have the expertise and the experience). The cost of redundancies for these staff who will mostly be immediately re-hired on new, possibly more costly contracts, is projected to be around £1bn19. Because spending £1bn to fire people who you will then pay the private sector to hire again is really smart.
In West London, a ‘pathfinder’ (ie preliminary) consortium has already bought in services from United Healthcare, the 2nd largest healthcare company in the United States, to run a ‘referral management’ service for them20. This means that when a GP writes a referral for a hospital or whatever, it will first have to go to a well-spoken American man with a briefcase and an interest in making shitloads of money to decide whether the referral should go through or not.
The NHS was founded to be a ‘free and comprehensive’ health service, but for the first time the CCGs will define what constitutes a health service, not the DH21, meaning there will be a postcode lottery of what service are available for free on the NHS in the area in which you live. As a result, ‘top up’ payments are being considered to force patients to pay for procedures outside of their definition22.
A commissioning group must arrange for the provision of services ‘as it considers appropriate’ – giving great leeway in how this is interpreted. There is still no duty to provide a comprehensive service on commissioning groups themselves. Similarly, attempts to improve openness and transparency are far too weak: get-out clauses would allow a commissioning group to avoid meeting in public if it ‘considers that it would not be in the public interest’, and a foundation hospital may exclude members of the public from meetings for unspecified ‘special reasons’.21
New commissioning groups, not the Secretary of State, will determine what actually constitutes the health service, potentially opening the door to “top-up” payments being charged for procedures that are outside their own definition of health services.
But top up charges are not the only worry. Rationing based on price (rather than need) will become widespread sooner and in more places than co-payments. The bond of trust vital in a functioning doctor-patient relationship will be put in jeopardy by the financial pressures and potential conflicts of interest whereby doctors may be forced to either deny needed care, or purchase unnecessary care respectively.
This brings me nicely to the hospitals or treatment centres which will be providing the questionably commissioned care. The Coalition’s health reforms are only half of the story here. Under New Labour, there had been a slow but steady increase in the number of non-NHS care providers commissioned by PCTs to do certain work.
These Independent Sector Treatment Centres (ISTCs) have attracted considerable criticism but were, in some cases, very wise choices indeed. ISTCs were originally intended to be sparingly applied in cases where for whatever reason NHS services were inadequate in order to give NHS services time to improve whilst the ISTC took care of some of the caseload to relieve pressure. NHS hospital running out of capacity? Don’t risk a bed-blocking crisis or a spike in waiting times, ship out elective surgeries to a local ISTC whilst the necessary investments are made at the NHS hospital. That sort of thing.
However, after a string of ultra-Blairite Health Secretaries under Blair and Brown (Alan Milburn, John Reid, Patricia Hewitt and to a certain extent Alan Johnson) relentlessly pushed the expansion of ISTCs they have become a small but permanent fixture in the NHS.
The Coalition’s plan is for an explosion in the use of private and voluntary sector providers, as well as forcing all NHS hospitals to become Foundation Trusts in April 2013 and then putting corporate rocket-boosters under them, opening up NHS hospitals for private management and the big bad market. NHS and private hospitals are expected to compete in an open market for referrals from CCGs.
As a necessary part of this process the health reforms have raised the cap on the proportion of private patients NHS hospitals are allowed to see to a whopping 49.9%. In 2010 private patient income represented just 0.6% of NHS income23. This will lead to a system whereby those with the cash (or the private insurance) are able to pay to jump the queue. The rich will be fast-tracked to the front of the queue for procedures meaning the poor will have to wait longer and longer for an NHS bed to become free24. Whilst this video is slightly out of date (removing the cap altogether was later amended to a 49.9% cap, which in practice will be exactly the same), it’s still a good illustration of the problem.
(note the truly Oscar-worthy acting from Labour’s parliamentary candidate for Cambridge and hence likely our next MP as ‘man in wheelchair’)
There are also damaging implications for the postgraduate training of NHS staff as private providers will have no obligation to engage in the level of costly hands-on experience for junior doctors that NHS trusts have done under SHA supervision25.
Nominally NHS hospitals will be victims of a range of pro-competition measures that will render their NHS status little more than a kitemark on a privately operated service. Foundation Trusts will be able to raise additional capital through loans, selling off assets and go through a new insolvency procedure if/when it all comes crashing down. Collectively these measures will allow the classic asset stripping tale to unfold, unleashing chaos in its wake: a swanky new management firm swoops in, makes unsustainable layoffs, sells assets, loads the FT up with highly leveraged debt and then scarpers with gargantuan fees and bonuses just before the entire financial house of cards collapses. This is exactly the model on which the Southern Cross care home collapse proceeded, a worrying precedent if ever there was one.
Concerns about predatory financiers aside, in any market system firms must be free to enter and exit the market. The government has claimed that certain oversight measures will prevent the worst excesses of the market and provide protection in the case of commercial failure. Despite this, there is the small matter of EU competition law to consider, with health minister Simon Burns himself stating that ‘as NHS providers develop and begin to compete actively with other NHS providers and private and voluntary providers, UK and EU competition laws will increasingly become applicable’21.
Whilst the full details of the commercial insolvency regime are yet to be known, the existence of EU competition law will more than likely mean an end to the government’s ability to bail out troubled hospitals. In other words, your local hospital may be sold off or shut down if it cannot keep its financials in order in a climate of chaos, cuts and competition. This is, rightly, rather an alien concept to most of us in the UK, but it is a real possibility. District General Hospitals could end up folding left right and centre, leaving the area they serve to the mercy of whatever private options the market deems profitable to run.
And the (very, extremely) limited evidence we have to go on so far seems to suggest that private hospitals and privately operated NHS hospitals may indeed struggle to provide the services the public accustomed to. Hinchingbrooke hospital in Huntingdon (where I was born!) has been under the franchise management of Circle Health for about a year now after Andrew Lansley signed off on one hell of a dodgy contract, and is losing money hand over foot as its deficit hits more than twice the projected level26 and was forced to ask for a cash advance27. In addition the patient satisfaction level has taken a decided turn for the worse28 and Circle’s ‘charismatic CEO’ Ali Parsa has walked away from the project altogether (with a £400,000 payoff, naturally) unexpectedly just days before answering questions before a committee of MPs29. If the hospital’s deficit rises from its current £4.1m to £5m then Circle are free under their contract to walk away and leave the hospital to collapse under which circumstances Peterborough and Adenbrooke’s hospitals would be forced to scramble together replacement capacity.
Of deep concern is how Monitor, the economic regulator of the entire flowcharty mess, is now going to function. Following outrage over its duty to ‘promote competition’, they must now ‘prevent anti-competitive practice’. No doubt the lawyers will have a field day with that one. Monitor and EU law could mean that NHS hospitals will be fined up to 10% of their turnover simply for cooperating with other local hospitals30.
But don’t take my word for it: the BMA, BOS, British Dental Association, British Geriatrics Society, British Psychological Society, Chartered Society of Physiotherapy, Community Practitioners and Health Visitors Association, CSP, GMB, Institute of Healthcare Management, Managers in Partnership, Patients Association, Royal College of GPs, Royal College of Midwives, Royal College of Nursing, Royal College of Paediatrics and Child Health, Royal College of Physicians of Edinburgh, Royal College of Psychiatrists, Royal College of Radiologists, Royal College of Surgeons, Society of Chiropodists and Podiatrists, Society of Radiographers, The Allied Health Professions Federation, UK Faculty of Public Health, Unison and Unite are with me on this too.

Fightback
However, all is not entirely lost. Campaigners with Keep our NHS Public in Gloucestershire managed to successfully reverse a decision to transfer 8 local hospitals out of the NHS, at the eleventh hour, keeping them instead in an NHS Trust through some legal skulduggery involving the complex rewriting of contracts with NHS trusts. Various Labour councils have been exploring similar methods with some success through the new Health and Wellbeing Boards (HWBs). Having said that, Monitor and local HWBs will no doubt frequently be at odds and I worry that Monitor may usually come out on top.
As Nye Bevan, the Labour MP who created the Health Service famously said, ‘The NHS will exist as long as there are folk left with the faith to fight for it.’
So, to recap:
- Dave repeatedly promised the voters that there would be no reorganisations
- The reasons offered for reform were bogus
- There are highly dubious relationships between the private healthcare lobby and the Coalition
- The reforms will herald the dawn of a massive new bureaucratic tangle which will have effects against the best interests of the patient
- The reforms have the potential for utter chaos if private contractors cannot deliver the savings promised
- The reforms place the principle of care free at the point of use at further risk
- A strong local campaign of resistance should (in theory) be able to mitigate the worst of these risks
The slow but irreducible erosion of the NHS’s founding principles of a universal, comprehensive and free health service is taking place in 2013. I call it privatisation, but for the patients who will be affected the words pain, fear and anger may seem to describe the situation just as well. Either way, it will be one of David Cameron’s most shameful legacies if we don’t mobilise to resist the changes locally and, above all, to elect a Labour government in 2015.
And finally, as a treat for those of you who have waded through so much verbiage to get here, and to lighten the mood, I present one of the best Downfall parodies I have ever seen:
I hope this mammoth undertaking makes up for the absence of blogging output recently…
- http://www.bbc.co.uk/news/uk-politics-12203000
- http://www.guardian.co.uk/uk/the-northerner/2012/feb/17/health-healthbill-simonburns
- http://www.guardian.co.uk/society/2012/dec/28/public-nhs-reforms-health-service
- http://www.guardian.co.uk/society/2011/aug/07/nhs-among-most-efficient-health-services
- http://www.kingsfund.org.uk/topics/nhs-reform/mythbusters/nhs-performance
- http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2010/Jun/1400_Davis_Mirror_Mirror_on_the_wall_2010.pdf
- http://www.kff.org/insurance/snapshot/OECD042111.cfm
- http://www.guardian.co.uk/society/2011/nov/07/nhs-cancer-figures-cameron-lansley
- http://www.leftfootforward.org/2011/11/cancer-not-the-only-story-of-improving-health-outcomes-under-labour/
- http://liberalconspiracy.org/2012/09/06/labour-goes-to-war-over-jeremy-hunts-views-on-nhs/
- http://www.tom-watson.co.uk/2009/04/daniel-hannan
- http://www.leftfootforward.org/2011/01/andrew-lansley-private-healthcare-supporters/
- http://www.leftfootforward.org/2011/01/andrew-lansley-private-health-no-surprise/
- http://www.leftfootforward.org/2011/06/andrew-lansley-nhs-reform-backers/
- http://www.powerbase.info/index.php/General_Healthcare_Group
- http://www.spinwatch.org/blogs-mainmenu-29/310-tamasin-cave/5435-the-nhs-will-be-shown-no-mercyq-says-cameron-health-adviser
- http://www.leftfootforward.org/2011/09/the-two-faces-of-nhs-reform/
- http://socialinvestigations.blogspot.com/2012/02/nhs-privatisation-compilation-of.html
- http://fullfact.org/factchecks/nhs_reform_reorganisation_costs_redundancies_labour-2778
- http://www.pulsetoday.co.uk/gp-pathfinders-linking-up-with-private-firms/11050155.article#.UPxNo2fkXkI
- http://www.unison.org.uk/file/Five%20reasons%20to%20scrap%20the%20bill.pdf
- http://skwalker1964.wordpress.com/2013/01/15/restricted-mckinsey-paper-portrays-grim-future-for-health-service/
- http://www.hi-mag.com/health-insurance/product-area/pmi/article378992.ece
- http://www.unison.org.uk/file/UNISON%20-%20Private%20Patient%20Income%20Cap%20briefing%20-%20Jan%202012.pdf
- http://www.leftfootforward.org/2011/05/the-effect-of-%E2%80%98liberating-the-nhs%E2%80%99-on-postgraduate-medical-training/
- http://www.managementinpractice.com/default.asp?title=Circle%5Fannounces%5F%A34m%5Fdeficit%5Fat%5FHinchingbrooke%5Fhospital&page=article.display&article.id=29488
- http://webcache.googleusercontent.com/search?q=cache:xPvWnzE1LPYJ:www.ft.com/cms/s/0/47eeb65c-1f5e-11e2-b2ad-00144feabdc0.html+&cd=1&hl=en&ct=clnk&gl=us#axzz2KRaHru3y
- http://www.mirror.co.uk/news/uk-news/hinchingbrooke-hospital-first-privately-run-nhs-1363151
- http://www.bbc.co.uk/news/uk-england-cambridgeshire-20672310
- http://www.guardian.co.uk/society/2011/apr/13/nhs-reforms-miliband-urges-government-scrap-bill
